From the Field
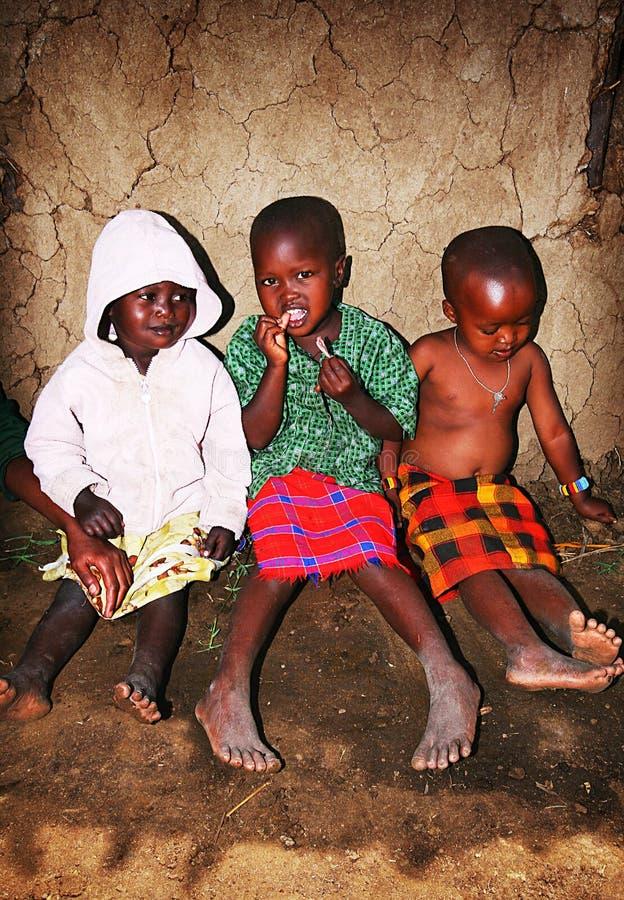
In rural Nigeria, a baby in severe respiratory distress died. Deserted by power, it stole her last breath.
Dr. Emmanuel Gayus, MPH, Harvard T.H. Chan School of Public Health
The Co-Founder
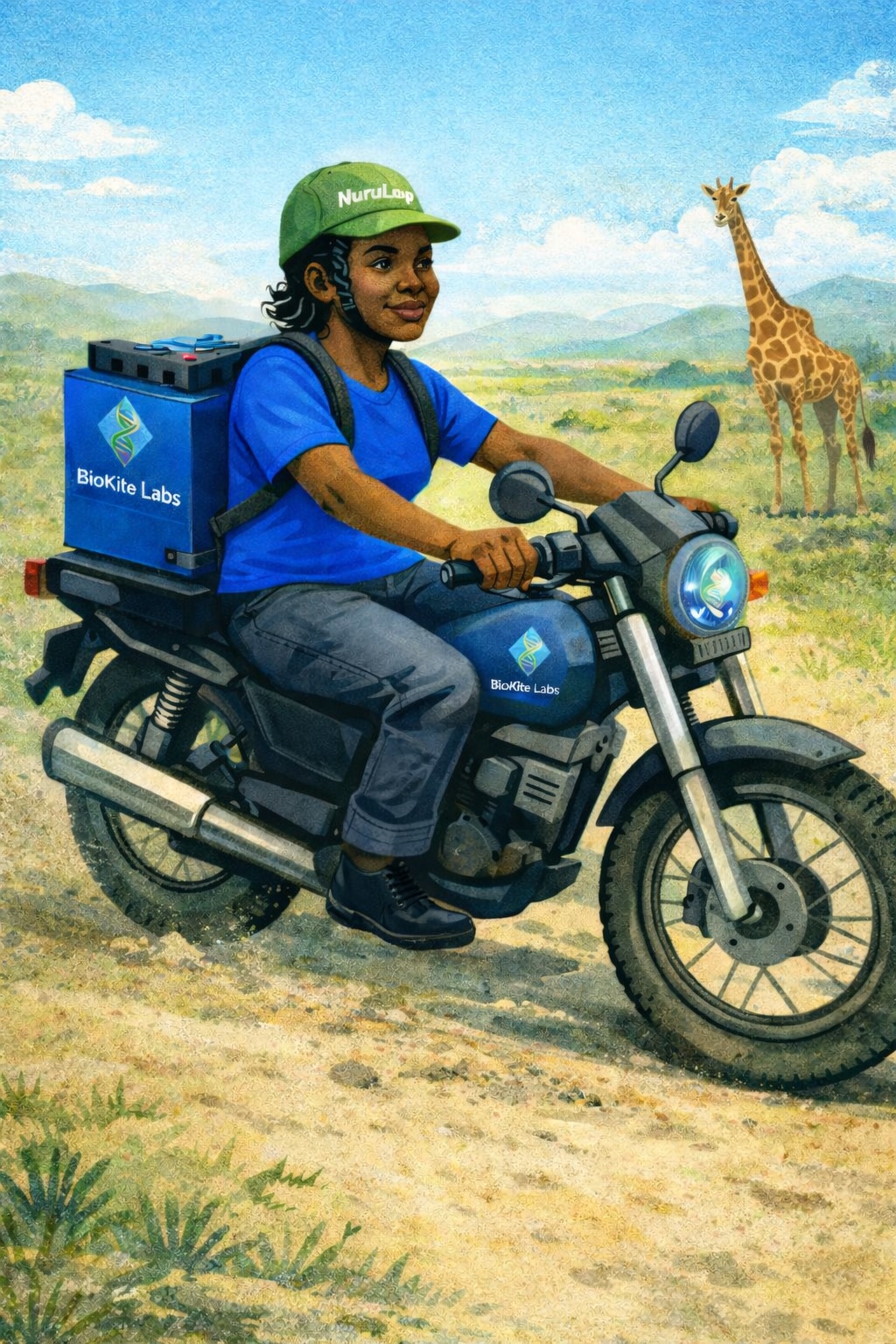
We delivered by phone light and transferred her 45km to the nearest hospital. With backup power, that transfer would not have been necessary.
Mike Tuffour Amirikah, MD MPH EMBA, Co-Founder & VP, BioKite Labs
The Founder
After losing my childhood best friend Penelope suddenly, with no warning she was severely ill, I understood what it means when the people around you cannot access the care they need. Communities in the Maasai Mara face that same reality every time a power outage hits during delivery.
Sarah Wang, MPH, Co-Founder & CEO, BioKite Labs